My approach to weight management
Why the way we think about weight has to change, and what that means now that medicine can finally act on the biology underneath it.
Why this matters
For most of medical history, weight has been treated as a test of character. Eat less, move more, and if it does not work, try harder. That model is not only unkind. It is wrong, and it has held back good medicine for decades.
Three things have changed at the same time. The science now shows clearly that body weight is biologically regulated, not a measure of discipline. A class of medicines, the GLP-1 receptor agonists, can act on that biology directly. And these treatments are increasingly available through digital health services that reach people a traditional clinic never would.
But access on its own is not care. A medicine handed over through a form, with no understanding of why it works or what happens when it stops, wastes most of its potential and can do harm. The approach matters as much as the molecule.
The shift in thinking
To use these medicines well, you have to change the question. The old question was how to make someone eat less. The better question is why the body defends a higher weight in the first place, and what it would take to change that.
GLP-1 medicines are not willpower in a pen. They are long-acting versions of a fullness signal the body already uses, working mostly in the brain's appetite circuits to lower the weight the body actively defends. Aimed only at the number on the scale, used like a faster crash diet, they disappoint. Used as a biological correction, inside a plan that treats the underlying condition and is built to last, they do something no diet has managed at scale.
Maximising their potential comes down to three shifts: treating obesity as the medical condition it is, working with the body's biology instead of against it, and planning for the long term instead of the quick result. Those three shifts are the pillars of how I practise.
How I practise

Treat the cause, not the effort
The number on the scale sits at the end of a long biological chain, not the start. Genes, development, hormones and environment interact to set the weight a body defends. Care should aim upstream, at the biology driving the defended range, not at the visible outcome of it.
Read the full analysis →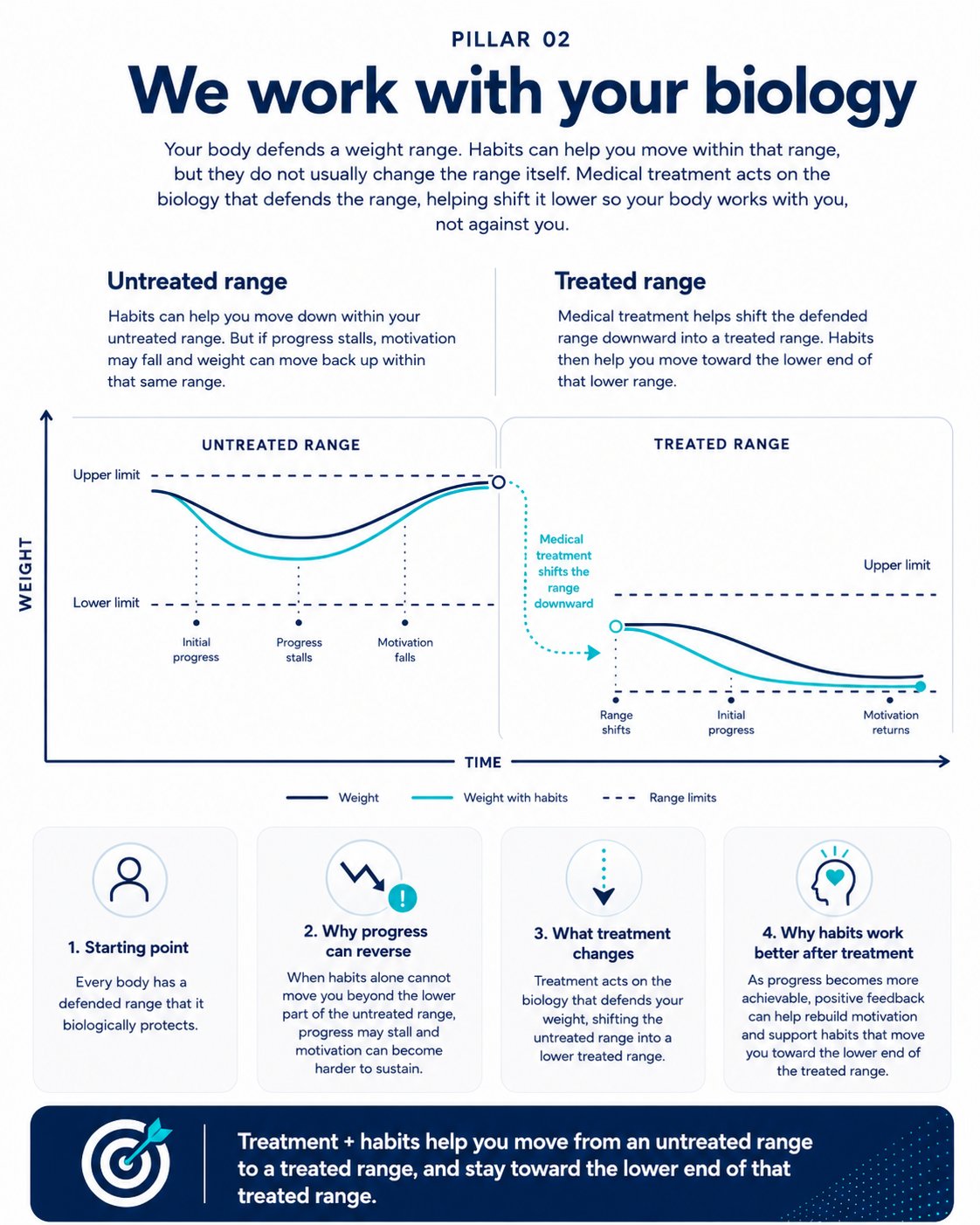
Work with the body's biology
Weight is a regulated variable the body defends. Lifestyle change moves a person within the untreated range but does not lower it. Medicine shifts that range down to a treated range. The body then stops fighting to return to its old weight, and the same habits that used to fail finally have room to work.
Read the full analysis →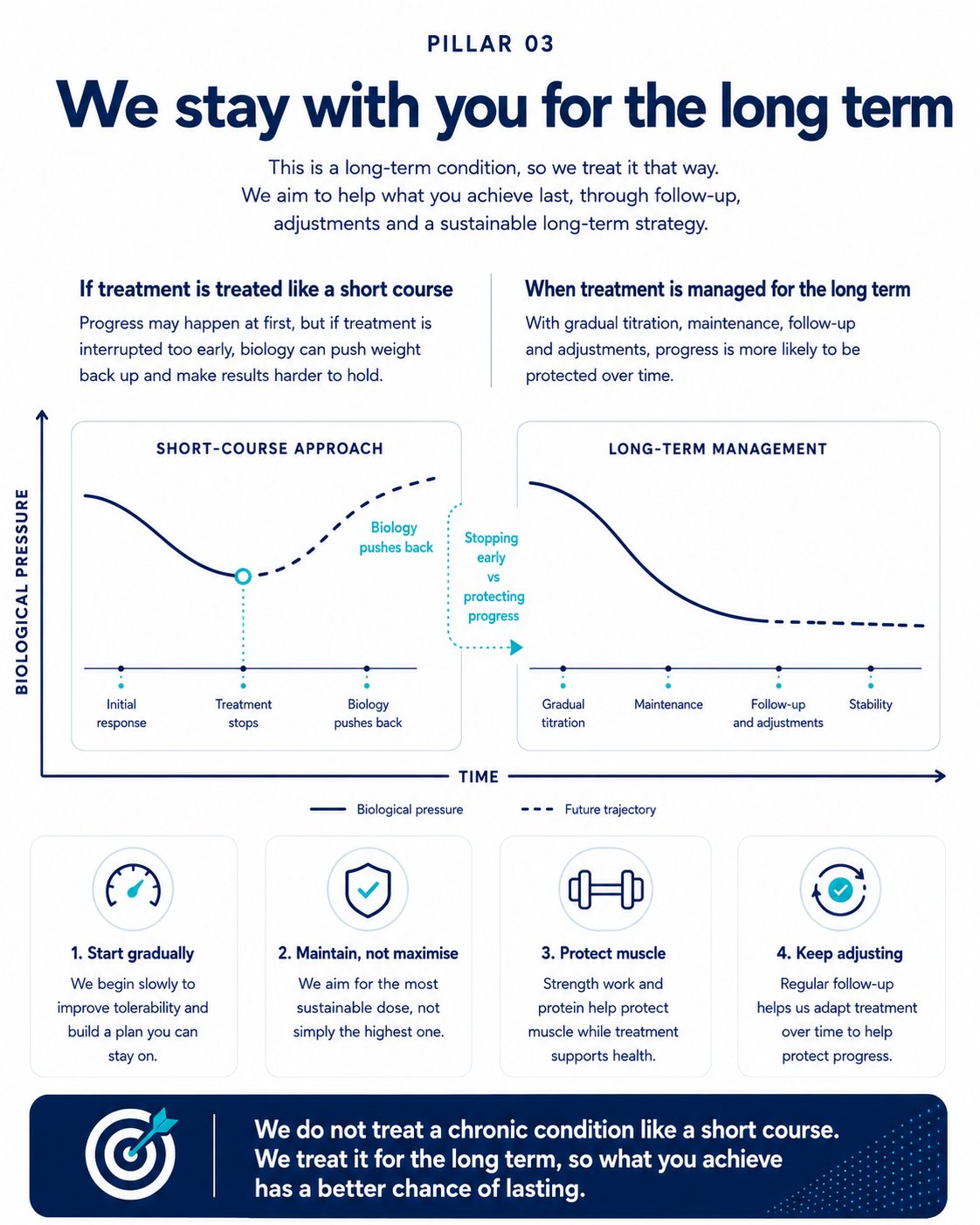
A long-term condition deserves long-term care
The biology that defends weight does not disappear once the weight comes down. Withdrawal studies show that when treatment stops, weight returns, just as blood pressure climbs when its medication stops. The goal is the lowest dose that holds the result, with the gains extending far beyond the scale.
Read the full analysis →What this means for digital health
None of this requires a clinic. It requires a way of thinking. A well-built digital service can deliver every part of it: an honest assessment of whether treatment is appropriate, a medicine matched to the person, education that explains the biology in plain language, and care that continues after the first prescription rather than ending with it.
That is the difference between selling a prescription and supporting someone through a long-term condition. These medicines are genuinely remarkable. They reach their potential only inside an approach that takes the condition, and the person, seriously.